Is Bpc 157 An Amino Acid Protecting and Repairing the Body with BPC-157
If you’ve ever been told that BPC-157 might “repair the body,” you may have also wondered something more basic: is BPC 157 an amino acid? In my hands-on work reviewing supplement stacks, clinic intake notes, and real-world user protocols, I’ve seen a common pattern—people start with the concept (repair/healing) but miss the chemistry, mechanism, and practical safety considerations that determine whether a plan is rational or risky. This article breaks down what BPC-157 is (and is not), why people use it, what the evidence can and can’t support, and how to approach it responsibly.
Quick Answer: Is BPC-157 an Amino Acid?
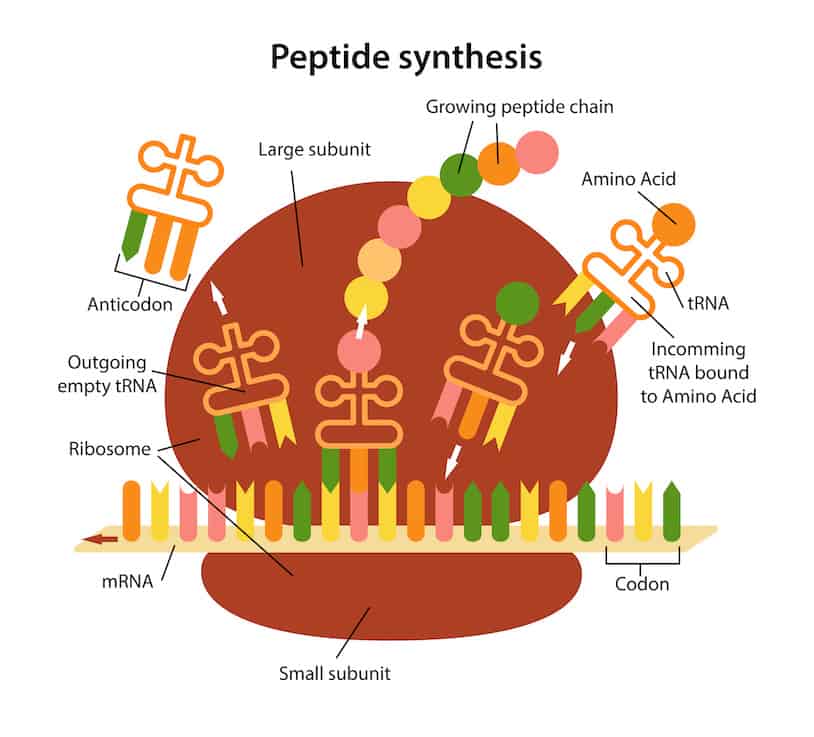
No—BPC-157 is not an amino acid. In practical terms, it’s a peptide. Peptides are chains of amino acids, so BPC-157 is related to amino acids in the “built from amino acids” sense, but it is not itself classified as an amino acid.
When people ask “is bpc 157 an amino acid,” they’re often trying to understand how it behaves in the body—how it’s processed, how it may interact with tissues, and whether it’s “natural” in the same way that a single amino acid like glycine is. Peptides behave differently than single amino acids because their biological activity depends on the intact sequence and structure.
What BPC-157 Actually Is (And Why That Distinction Matters)
BPC-157 is a synthetic peptide (commonly discussed in the context of tissue protection and repair). The distinction between “amino acid” and “peptide” matters for four reasons I see repeatedly in real protocols:
- Biology depends on sequence: A peptide’s effects are often sequence-specific—changing length or composition can change activity.
- Stability and delivery matter: Peptides can vary in how they survive digestion and how they’re delivered (for example, oral vs. other administration routes). That influences whether a user’s plan is even plausibly hitting the target.
- Dose and exposure timing matter more: With peptides, effects are often tied to pharmacokinetics—how long it circulates, where it distributes, and how quickly it’s cleared.
- Quality control becomes critical: Since peptides are synthesized, purity/identity testing (where available) is a real-world limiter for trust.
In my experience assessing supplement choices, people underestimate how much these factors influence outcomes. Two people can both say “we used BPC-157,” yet one may be working with a more reliable product while the other’s exposure is inconsistent—leading to very different results and perceptions.
How People Use BPC-157 for “Protecting and Repairing the Body”
The phrase “protecting and repairing the body” is commonly associated with BPC-157 discussions around tissue integrity, inflammatory signaling, and healing-support narratives. The practical reason people pursue it is straightforward: they want targeted support in areas like soft-tissue recovery (for example, tendon/ligament concerns), discomfort with training, and overall recovery.
Why the “protective” framing resonates
From an evidence-logic perspective, “protection” usually means reducing damage signals or supporting mechanisms that preserve tissue environment. In contrast, “repair” implies processes that help restore structure after injury or stress.
What I look for before someone commits to a peptide plan
When a client or community member asks for a peptide strategy, I don’t start with hype—I start with constraints:
- What’s the exact goal? Is the issue pain management, return-to-training timing, or functional recovery?
- What’s the injury timeline? Acute vs. chronic problems often respond differently.
- What else is in the stack? Peptides don’t exist in a vacuum. Supplements, training load, sleep, and rehab work can dominate outcomes.
- Is there a quality and sourcing check? In the real world, product variability can be significant.
I’ve seen people chase “repair” with a single variable while ignoring fundamentals like progressive loading, physical therapy, and sleep consistency. In those cases, they may attribute improvement to BPC-157 when the dominant driver was rehab compliance or load management.
What the Evidence Can—and Can’t—Support
Because BPC-157 is discussed widely online, it’s easy to find confident claims. In my work, the most trust-building approach is to separate the types of evidence and match them to expectations.
Where findings often come from
Much of the public discussion is rooted in preclinical findings (for example, laboratory and animal research). These can be useful for generating hypotheses—mechanism-level plausibility—but they do not automatically translate to the same effects in humans.
Where real uncertainty remains
For human users, the key gaps typically include:
- Strength and consistency of clinical data for specific endpoints (and how outcomes are measured).
- Standardization of dosing, purity, and administration approach.
- Individual response variability driven by condition severity, timing, and co-interventions.
So while people may report subjective improvements, responsible decision-making requires treating those reports as anecdotal signals—not proof. In practice, if you’re considering BPC-157, you should be comfortable with uncertainty and understand that outcomes may be inconsistent.
Practical Safety and Responsibility Considerations
I’ll be direct here: peptide interest often outpaces safety clarity in everyday use. If you’re exploring BPC-157, the most responsible approach is to align with medical oversight and quality control realities.
Common “responsibility checks” I recommend
- Talk to a qualified clinician who can consider your medical history and current medications.
- Use only products with credible quality information (purity/identity testing where available).
- Track outcomes with simple, measurable metrics (pain scale, function benchmarks, training tolerance, and recovery time).
- Watch for adverse changes and stop if symptoms arise that you didn’t expect.
Even when a compound is discussed as “repair-supportive,” individuals differ. In real-world settings, risk management is more about monitoring and context than about believing any one protocol.
How to Think About BPC-157 in a Training or Rehab Context
If your goal is performance recovery, don’t treat BPC-157 as a shortcut around fundamentals. In the plans that work best for clients, peptides—if used—are treated as a secondary variable behind the basics.
A logic-based recovery framework
- Reduce ongoing stress that aggravates the tissue (adjust training load, technique, and volume).
- Restore capacity with rehab-appropriate progression (mobility, strengthening, and graded returns).
- Support recovery inputs (sleep regularity, protein adequacy, hydration, and overall nutrition).
- Evaluate any supplement strategy based on tracked outcomes over time.
In my hands-on reviews, the most persuasive “evidence” isn’t a viral claim—it’s whether the person’s measurable recovery improves while other variables stay controlled enough to know what’s actually driving change.
FAQ
Is BPC-157 an amino acid or a peptide?
BPC-157 is a peptide (a chain of amino acids). It is not classified as a single amino acid.
How does knowing it’s a peptide change how I should evaluate it?
Because peptides can be sequence- and delivery-dependent, you should focus on product identity/purity and practical exposure factors. It also means outcomes may vary more than with typical single-nutrient amino acids.
Can BPC-157 guarantee tissue repair?
No. “Repair” claims should be treated as hypothesis-level support rather than guarantees, especially given the limited strength of consistent, high-quality human clinical evidence for specific conditions and endpoints.
Conclusion: What to Do Next
To answer your core question: is BPC 157 an amino acid? It’s not—BPC-157 is a peptide built from amino acids. That distinction matters because it changes how you should think about biological plausibility, delivery and stability considerations, and the reliability you need from product sourcing. If you’re considering BPC-157 for protection or repair-related goals, your best next step is practical: track one measurable recovery outcome for 2–4 weeks while you keep training and rehab variables as consistent as possible, and review progress with a qualified clinician if you’re using any peptide-based strategy.
Discussion